
SSG TEST: THE FERTILITY SCAN
What Is the SSG Test?
When a couple struggles to conceive — or when a woman experiences recurrent miscarriage or repeated IVF failure — one of the most important yet frequently overlooked investigations is the SSG test, also known as Saline Sonohysterography (SHG) or Saline Infusion Sonohysterography (SIS). This straightforward, minimally invasive procedure provides a detailed view of the inside of the uterine cavity — the space where an embryo must implant and grow — and is one of the most valuable diagnostic tools in modern fertility medicine.
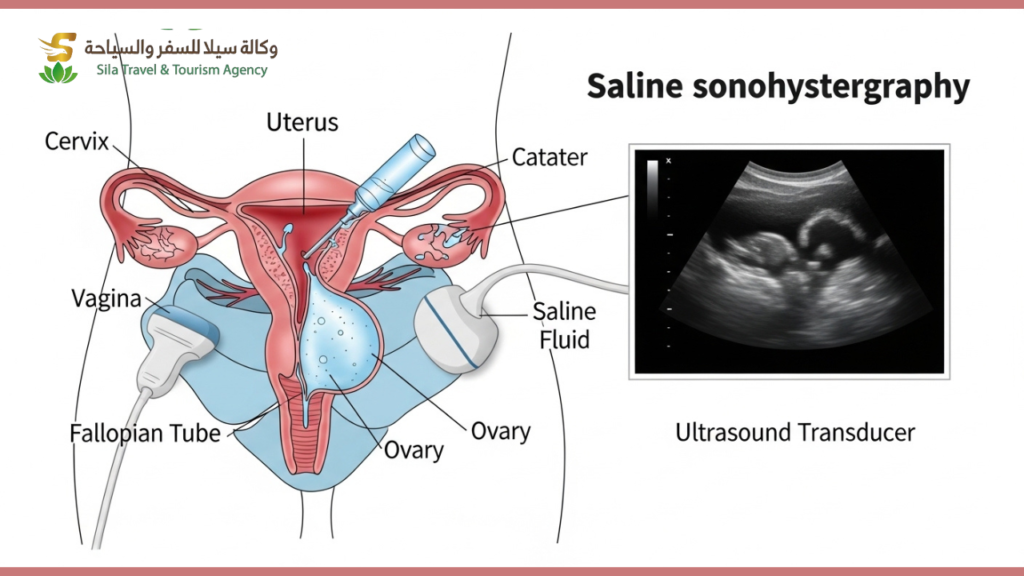
In simple terms, the SSG test is an enhanced ultrasound of the womb. A small amount of sterile saline solution (salt water) is gently introduced into the uterine cavity through a thin catheter, causing the cavity walls to separate and become clearly visible on ultrasound. This allows the fertility specialist to detect abnormalities inside the uterus that a standard transvaginal ultrasound cannot reliably identify.
At Sila Med Tour, we ensure the SSG test is included as a key part of the complete fertility evaluation we coordinate for our patients from the GCC and Africa — because an undetected uterine abnormality is one of the most common and correctable causes of failed IVF and recurrent pregnancy loss.
Why Is the SSG Test Performed?
The uterine cavity must be perfectly receptive for an embryo to implant successfully. Any structural abnormality inside the womb — no matter how small — can physically prevent implantation, disrupt early development, or cause miscarriage. The SSG test is specifically designed to identify these abnormalities with high accuracy.
It is recommended for women who have experienced two or more failed IVF or IUI cycles, recurrent miscarriage (two or more pregnancy losses), unexplained infertility despite normal basic investigations, abnormal uterine bleeding or irregular periods, or suspected uterine abnormality on a previous standard ultrasound.
The SSG test is particularly valuable because it detects conditions that a routine transvaginal ultrasound frequently misses — including small polyps, subtle fibroids projecting into the cavity, and mild adhesions — all of which can silently sabotage fertility.
What Can the SSG Test Detect?
A well-performed SSG test can identify a comprehensive range of uterine abnormalities:
Endometrial Polyps are the most commonly detected finding. These are benign growths of the uterine lining that can interfere with embryo implantation. They are estimated to be present in up to 32% of women with unexplained infertility and are frequently invisible on standard ultrasound. Polypectomy (surgical removal) has been shown to significantly improve natural and IVF conception rates.
Submucosal Fibroids are uterine fibroids that protrude into the uterine cavity. Unlike fibroids located within the uterine muscle or on its outer surface, submucosal fibroids have a direct and significant negative impact on implantation and pregnancy rates. Their identification and removal before IVF substantially improves outcomes.
Intrauterine Adhesions (Asherman’s Syndrome) are bands of scar tissue inside the uterine cavity, most commonly caused by previous uterine surgery, dilation and curettage (D&C), or infection. Adhesions reduce the functional surface area of the endometrium and are a well-recognised cause of recurrent miscarriage and infertility.
Uterine Septum is a congenital abnormality where a band of tissue divides the uterine cavity partially or completely. It is the most common uterine structural anomaly and is strongly associated with recurrent miscarriage. A septum is identified on SSG and confirmed with 3D ultrasound or hysteroscopy.
Irregular or Thin Endometrium — the SSG test evaluates the texture and uniformity of the uterine lining, providing additional information about endometrial receptivity beyond what thickness measurement alone can offer.
What Does the Procedure Involve?
The SSG test is a simple outpatient procedure that takes approximately 15–30 minutes and requires no general anaesthesia.
It is ideally performed between Day 6 and Day 10 of the menstrual cycle — after menstrual bleeding has stopped but before ovulation — to ensure the endometrium is thin and the cavity is easiest to visualise.
A speculum is gently placed in the vagina, and the cervix is cleaned. A thin, soft catheter is then passed through the cervix into the uterine cavity. The speculum is removed, and a transvaginal ultrasound probe is inserted. Sterile saline is slowly introduced through the catheter while real-time ultrasound images are captured as the fluid fills and outlines the uterine cavity. The entire cavity is systematically examined and any abnormalities are documented.
Most women describe the procedure as similar to period cramping — mild to moderate discomfort that passes quickly. Taking a standard painkiller such as ibuprofen 30–60 minutes before the procedure is usually sufficient. Women with cervical stenosis (a narrow cervical canal) may experience more discomfort, and their doctor should be informed in advance.
SSG vs. HSG: What Is the Difference?
Patients are sometimes confused between the SSG test and the HSG (Hysterosalpingography) — another common uterine investigation. Understanding the difference helps clarify when each test is appropriate.
| Feature | SSG Test | HSG |
| Medium used | Sterile saline | X-ray contrast dye |
| Imaging method | Ultrasound | X-ray (fluoroscopy) |
| Best for | Uterine cavity abnormalities | Fallopian tube patency |
| Radiation exposure | None | Yes |
| Detail of cavity | Superior | Moderate |
| Fallopian tubes | Not assessed | Assessed |
In many fertility centres, both tests are performed as part of a complete female fertility work-up — the SSG for detailed cavity assessment and the HSG for tubal evaluation. Sila Med Tour coordinates both investigations as part of a seamless pre-treatment diagnostic package.
Why GCC and African Patients Particularly Benefit From the SSG Test
Uterine fibroids are significantly more prevalent in women of African descent — studies consistently show rates two to three times higher than in other populations. Many of these fibroids are submucosal and directly impact fertility, yet they are frequently undetected until a woman has already experienced multiple failed IVF cycles or miscarriages.
Similarly, Asherman’s syndrome — uterine scarring from previous D&C procedures — is underdiagnosed across both GCC and African patient populations, where access to specialist hysteroscopic evaluation has historically been limited.
Medical tourism through Sila Med Tour ensures patients receive the SSG test as a standard part of their fertility evaluation — performed at internationally accredited centres equipped with high-resolution ultrasound technology and reported by experienced reproductive specialists — before any IVF investment is made.
Take the First Step
If you have experienced failed IVF cycles, recurrent miscarriage, or unexplained infertility, the SSG test may reveal the answer that has been missing from your investigations. It is a simple, safe, and highly informative procedure that could be the key to unlocking your path to parenthood.
Faqs
No FAQs found.
Get Free Medical Consultation
Fill the form and our team will connect with you instantly.